There is a specific kind of “confusion” that stems from a system designed to be opaque. For decades, the American healthcare apparatus has operated behind a veil of complex billing and “regulatory capture”—a term that sounds academic until you realize it’s the reason your medical bills are skyrocketing while your time with an actual doctor is shrinking.
My fellow Substacker and health care enlightener, Dutch Rojas, recently did a brilliant job recently explaining the traps of regulatory capture and how this has happened to the health care market.
Not everyone following me here is a patient at my practice, but for twenty years, I have been sounding the alarm. I have watched firsthand how, via Medicare payment policy, the government has systematically torn down the profession of medicine, replacing the physician-patient bond with a managed industrial complex.
The single most leveraged moment resulting in true market siphoning and the total disruption of traditional physician led health care came with the legislated agreement to price-fix physician payment within Medicare.
The RVU (Relative Value Unit) system was created in 1989 (implemented 1992) to replace chaotic, inflationary physician billing with a standardized, resource-based payment model—but in doing so, it laid the groundwork for today’s administratively driven, volume-measured healthcare economy. One of the strongest arguments for using this system was that physician knowledge and thinking skills were undervalued and procedural care was “arbitrarily” being overvalued in the marketplace.
Ironically, the result of the RVU codification of physician services has only further distorted payment towards technical procedural pay over physicians’ relative value. If one were to analyze the payment provided in this program, the facility and technical components of a point of care is rewarded a far higher dollar payment than the physician providing the actual care or diagnostic interpretive skillset. The idea of regulatory capture is obvious when the stated argument for the need of policy resulted in actually worsening the problem.
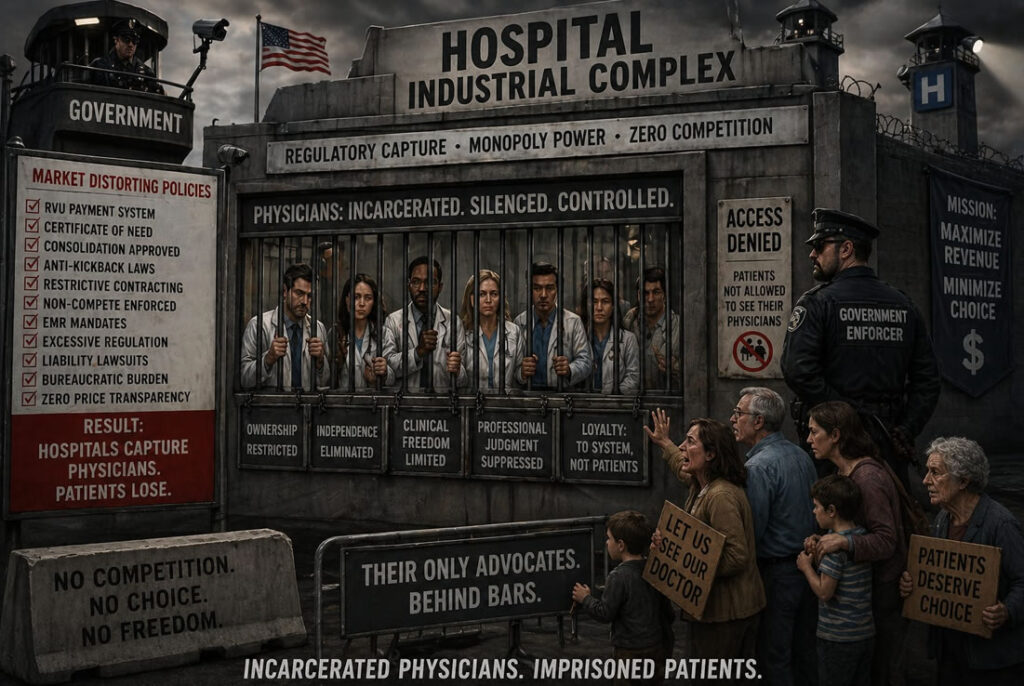
Dutch Rojas’s article goes on to demonstrate how Stark Regulation (preceded the RVU system) resulted in legislating the formal removal of physician ownership of any service outside their direct license and location of care. Then as time went on, government policy continues to progressively add more market distorted payment policies and regulatory restrictions which has enabled Hospitals to regulatorily capture nearly all physicians. By incarcerating us, hospitals have caused patients to lose their only true advocate and healers.
Not everyone following me here is a patient at my practice, but for twenty years, I have been sounding the alarm. I have watched firsthand how, via Medicare payment policy, the government has systematically torn down the profession of medicine, replacing the physician-patient bond with a managed industrial complex.
As more discussion in social media keeps pointing out the opaque and unfair payment schemes experienced by average citizens it is becoming more obvious that a day of reckoning is inevitable. If you are on X, nearly daily Mark Cuban, millionaire entrepreneur who started his Cost Plus generic medication virtual pharmacy is drilling deeper and deeper into the “insane” and illogical payment schemes built into our system. He still hasn’t come to the full conclusion that the free market is how this gets resolved. From some of his comments, I feel he is falling into the trap that keeping this a political issue (perhaps he has sights on running for office) remains the way for change. I disagree.
The best thing that could happen in my view is that the present administration and congress keeps moving towards liberating the control of health care dollars back into the hands of the citizen. We need to end mandated insurance and we need to stop discriminating against those trying to refuse paying for mandated insurance.
Health insurance is a failed product and the evidence is to note how many Americans are getting subsidized in order to “afford” the service. The ACA marketplace is no longer a traditional insurance market—it is a government-subsidized purchasing system where ~92–93% of participants rely on federal premium support. Over 22 million of 23-24 million enrollees. This is a failed policy pure and simple.
The single most discriminatory regulation presently in place is forcing high- deductible insurance purchases in order to allow an individual to have Health Savings Accounts. We need to allow Health Savings Accounts to any tax-paying US citizen of adult age.
Instead of borrowing more money or returning Medicare beneficiaries back to the added tax turnstile, we need to allow Medicare retirees to transfer IRA and pension savings/profits toward their own HSA. Stop using the RVU Medicare payment scheme as the cash register for and market arbitrator for health care innovation and price determination.
This past January I exposed a clear example of how Regulatory Capture gets done. It was my post regarding the special payment and waiver provided to Hospitals during the COVID debacle. Congress has just extended this “experiment”. What is most revealing about this story is that the update on the safety of virtual hospital care is that the data is an admission that a large amount of hospitalization appears unnecessary.

This past January I exposed a clear example of how Regulatory Capture gets done. It was my post regarding the special payment and waiver provided to Hospitals during the COVID debacle. Congress has just extended this “experiment”. What is most revealing about this story is that the update on the safety of virtual hospital care is that the data is an admission that a large amount of hospitalization appears unnecessary.
To my understanding there is no intent for congress to open up the Virtual Hospital concept to Medicare physicians. The irony of all this policy is that hospitals which should becoming less necessary for most of our healthcare are being incentivized to move into your bedroom AND get paid as if they built you a hospital suite.

Clearly they plan on running with this new regulatorily captured market.
Last week I wrote about Medicare’s “virtual hospital” experiment and a simple observation that followed from it: much of what we call inpatient medicine does not appear to require a hospital building at all. When patients with pneumonia, heart failure exacerbations, cellulitis, COPD flares (acute on chronic lung impairment), and similar conditions were …
And As The Lyrics Go:
Yesterday’s glory won’t help us today
You wanna retire?
Get out of the way
I ain’t got much time
The young ones close behind
I can’t wait in line
If we can not wake you
Then we’ll have to shake you
Disclaimer: This information is for educational purposes only and is not intended to replace professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.
Step away from fragmented, institution-driven healthcare and build a direct relationship with a physician who knows your history and advocates for your needs. Schedule a complimentary consultation with our concierge physicians to discover a more personal and coordinated approach to care.
Southwest Florida’s premier Medical Home. Dedicated to prevention, access, and the patient relationship. Serving Fort Myers, Sanibel, Cape Coral, Bonita Springs, Naples, Punta Gorda & surrounding Southwest Florida areas.
Contact
6160 Winkler Road
Fort Myers, FL 33919
(239) 362-3005
Fax: (239) 362-3392
staff@imlwp.com