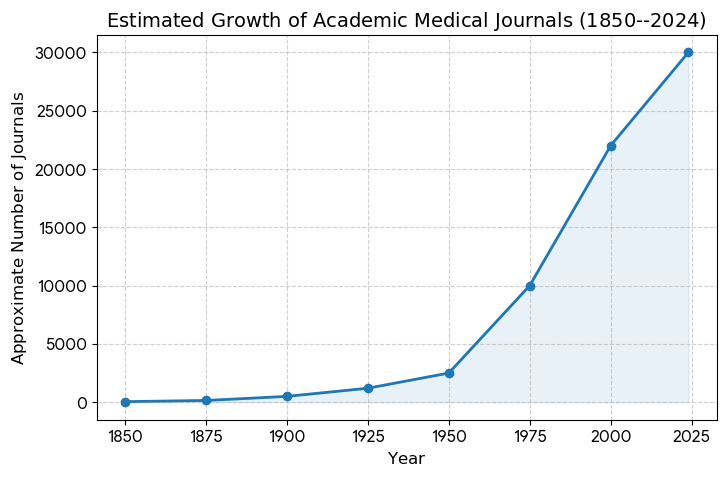
I think it appropriate for the public to try grasping how much research is published for the medical community.
According to Google AI, for U.S. physicians, the following are currently considered the most reputable and widely referenced “big” journals:
New England Journal of Medicine (NEJM): Established in 1812, it remains the most prestigious peer-reviewed medical journal, particularly for clinical trials and original research.
Journal of the American Medical Association (JAMA): A staple for U.S. practitioners, providing broad editorial coverage and highly cited peer-reviewed articles across all medical disciplines.
The Lancet: While based in the UK, it is globally influential and a primary reference for international health and significant specialty research.
The BMJ (British Medical Journal): Known for its rigorous standards and focus on medical education and clinical practice.
Annals of Internal Medicine: The official journal of the American College of Physicians, highly regarded for its focus on Internal Medicine and healthcare policy.
Nature Medicine: Often cited for translational research and breakthroughs that bridge the gap between basic science and clinical application.
I will say that the Journal of American Medical Association has become the rag for international healthcare policy with an occasional real scientific article. They worked hard at sabotaging COVID treatment studies during the Pandemic (aka Plandemic). In my view, JAMA is a government mouth piece touting medically irrelevant “wishes” of international health care policy. The journal totally misses the fact that health care populations are local and regional and it is a Prometheus effort to force universal standards to our country.

Likewise, the NEJM provides an excessive academic representation in their opinion articles. This journal does still offer more rigorous research articles and excellent reviews of medical diseases.
The Lancet and British Journal of Medicine (BJM)- British publications- need I say more??
Annals of Internal Medicine. Historically a great journal and in my opinion, the most reliable journal for real scientific inquiry. It is born from the American College of Physicians. Granted, they too, have fallen prey to certain political biases but they are still scientifically the more rigorous of the present modern day medical journals.
Nature Medicine??? Not a physician read journal. It is, however a good source for bench research. Bench research is hypothesis generating BUT not necessarily clinically relevant.
The American Journal Of Medicine. This “Top 3 U.S Medical journals” was placed into the ash heap of the internet search options when Dr. Peter McCullough offered to clinicians the COVID Outpatient Treatment Protocol. I have always considered this medical journal worthy of my precious reading time.
My readers know I have reported on the myth vs science of coffee and caffeine. Here again is a recent article addressing a common question. “Should I stop drinking coffee now that I have a diagnosis of Atrial Fibrillation ( a form of rapid and irregular heart beats).
The DECAF Randomized Clinical Trial (November 2025) disputes the myth that coffee causes heart arrhythmias, finding that daily consumption may actually reduce atrial fibrillation recurrence by 39%. Furthermore, studies indicate that moderate coffee intake is associated with lower risks of heart failure and stroke, while encouraging physical activity. Read the full story at UCSF News.
For years, many doctors and patients believed that caffeine was a “trigger” for heart rhythm issues like Atrial Fibrillation. However, recent clinical evidence suggests the opposite may be true for many people.
Traditionally, it was thought that caffeinated coffee was proarrhythmic (meaning it promotes irregular heart rhythms). The DECAF trial was specifically designed to test this theory by comparing patients who drank coffee to those who avoided it entirely.
The study found that patients who had recently undergone treatment for persistent AF (cardioversion) actually fared better when they consumed coffee:
Coffee Group: Only 47% had a recurrence of AF within six months.
Abstinence Group: 64% had a recurrence of AF within the same timeframe.
The Result: Drinking at least one cup of caffeinated coffee daily was associated with a 39% lower hazard of the arrhythmia returning.
While the study focused on the results rather than the biological “why,” researchers and the AHA often point to several ways coffee may protect the heart:
Antioxidant Properties: Coffee is a major source of antioxidants, which can reduce inflammation and “remodeling” of the heart tissue.
Adenosine Blocking: Caffeine blocks adenosine receptors; since adenosine can sometimes shorten the heart’s electrical recovery period (potentially triggering AF), caffeine may provide a stabilizing effect.
Improved Heart Health: Regular consumption has been linked to lower risks of other heart-related issues, which indirectly keeps the heart’s electrical system healthier.
Diabetes is a well established associated condition with acute myocardial infarction (heart attack). Recent articles are confirming a mild increased incidence of the medical definition of diabetes with the use of statin medications prescribed for cholesterol lowering in at risk patients.
A recent study confirmed that the benefits of statin prescription in diabetic patients clearly outweighed any risk of medication use. In fact, ALL CAUSE mortality was benefited in the Statin group.
This is an important and might I say and ADDITIVE study supporting cholesterol lowering in high risk patients for coronary and other macrovascular events.
Note- the myth that statins promote liver disease and medically relevant harm is again refuted in this study. I am really tired of patients reporting their “literature” social feeds “notices” that using proven lipid lowering medication is harmful.
A recent study looking at analyzing common genetic variants associated with coronary artery disease confirms that the lion’s share of at risk coronary artery events is “POLYGENIC” versus single gene associated. This review is interesting to me because it demonstrates how the heart disease problem early on was assessed through familial inheritance patterns.
That research led to the now proven hypothesis that elevated LDL cholesterol resulted in early death from coronary occlusion of cholesterol burdened plaques and associated thrombosis. Heterozygous and homozygous hypercholesterolemia are the two primary pedigrees of this association.
Doctors can find these patient subjects by measuring the phenotypical presentation- namely LDL cholesterol levels in the 95th percentile or higher. If these values are further linked with family histories of early heart attacks, the diagnostic certainty rises to very high levels.
That research led to the now proven hypothesis that elevated LDL cholesterol resulted in early death from coronary occlusion of cholesterol burdened plaques and associated thrombosis. Heterozygous and homozygous hypercholesterolemia are the two primary pedigrees of this association.
Doctors can find these patient subjects by measuring the phenotypical presentation- namely LDL cholesterol levels in the 95th percentile or higher. If these values are further linked with family histories of early heart attacks, the diagnostic certainty rises to very high levels.
So far studies confirm that in most cases it is a multitude of genetic variants that additively contribute to early heart attack risk. Unfortunately as of now, the concept of incorporating across the board genetics analysis to risk predict high risk patients has very low yield. I suspect that with time and especially with quantitative computing the precision of genetic analysis will eventually become clinically useful. Even though there are multiple genetic associations that are not directly linked to LDL cholesterol, LDL lowering lowers events in polygenetic high risk patients.
rom genetic reported information when an individual has a polygenic risk (family history), it turns out behavior/lifestyle changes have an equal positive benefit for outcome as medical intervention. THIS MEANS, IN THE CONTEXT OF A POSITIVE FAMILY HISTORY OF EARLY HEART ATTACK, CURRENT MEDITERANIAN DIET AND ACTIVITY RECOMMENDATIONS WORK AS WELL AS MEDICATION INTERVENTION. LIKEWISE ALL MEDICATION TRIALS ASSESSING LDL CHOLESTEROL LOWERING SHOW CLINICAL BENEFIT FOR CARDIAC EVENTS AND ALL CAUSE MORTALITY. WHAT ISN’T KNOWN BASED UPON CURRENT LITERATURE IS WHETHER COMBINING LIFESTILE CHANGES WITH LDL LOWERING MEDICATIONS IS SUPERIOR TO EACH INDIVIDUAL APPROACH.
Disclaimer: This information is for educational purposes only and is not intended to replace professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.
Southwest Florida’s premier Medical Home. Dedicated to prevention, access, and the patient relationship. Serving Fort Myers, Sanibel, Cape Coral, Bonita Springs, Naples, Punta Gorda & surrounding Southwest Florida areas.
Contact
6160 Winkler Road
Fort Myers, FL 33919
(239) 362-3005
Fax: (239) 362-3392
staff@imlwp.com