Recently a prescient article from Dr. Jane Orient MD, reviewing the skin organ and clinical manifestations of Covid 19 vaccines, got me contemplating the interrelationship of several Internal Medicine “disciplines” and actual patient presentations.
Beginning just about 2 weeks ago, while I have been contemplating what I have been learning since the COVID 19 pandemic and immunity, I came across Dr. Orient’s review on the skin organ system. Since COVID 19, I have been slowly digesting functional immunology concepts new to my traditional allopathic medical training, as well as looking into more of a system’s biology approach to patients health and disease.
Then comes Dr. Orient’s article. Brilliant as always. I keep her, Sapira’s Art and Science of Bedside Diagnosis in my home office library. I consider Dr. Orient razor sharp and objectively the most efficient physician and patient advocate in our generation.
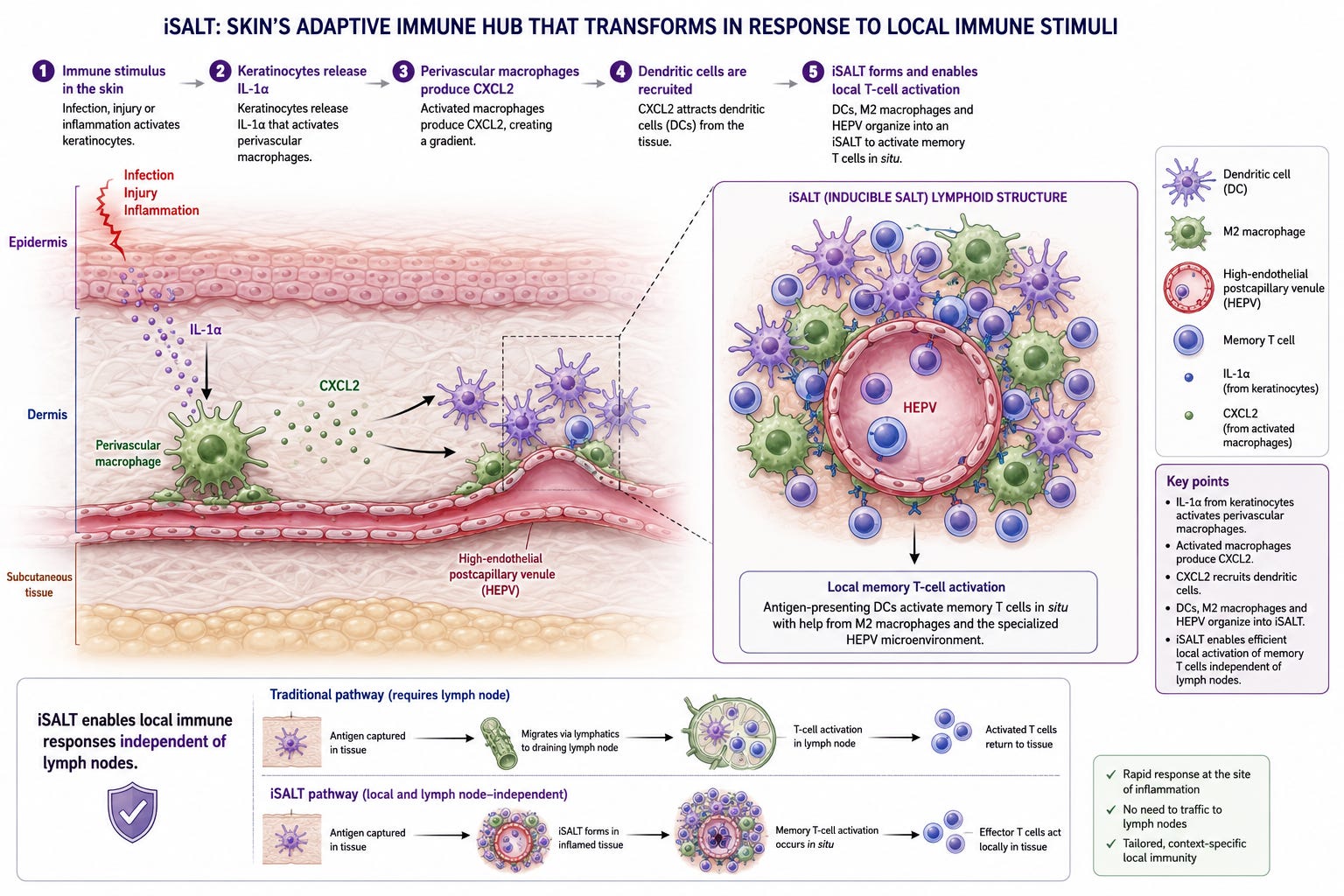
Following is a graphic of how our skin organ, starting as a protective barrier to our more fluid and susceptible internal physiology, can actually harness an acute immune and neurologic transformation in response to external environmental insults.
A local self-employed business owner, aged appx 60 years, found our practice on the internet. His primary physician recently retired. The patient was told approximately three years ago that his cholesterol panel was unhealthy. His primary concern and focus was that he had elevated triglycerides which were getting steadily worse despite him modifying his diet. He has a near ideal body weight but had a bit of excess intrabdominal fat distribution.
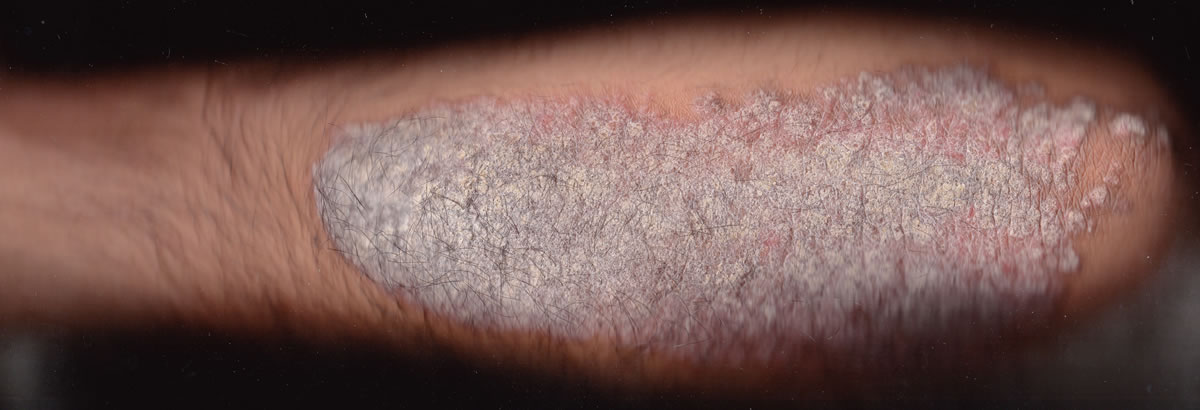
He was aware of a diagnosis of psoriasis for decades and found topical management difficult. Upon examination, he clearly had a fairly high burden of psoriatic plaques on his arms, legs and some small patches on his trunk.
He reported his doctor advised a statin based upon his lipid trends. His doctor recognized his overall profile placed him at higher risk for a heart attack from his age-matched peers. He wanted to know what he could do lifestyle wise to improve his profile and risk. He also reported reading in the AI engines that there was a relationship with his triglycerides and psoriasis. This claim was new to me.
Upon history and other lab measurements including the Prism Io antioxidant device, it was clear he could make significant nutritional and dietary changes that should improve his cholesterol profile. Losing 5-10 pounds of fat with a focus on lowering visceral fat would also help the situation. I explained how an enzyme called LPL (lipoprotein lipase) was lacking certain inputs for optimal functional activity. For this patient this included diet changes to lower insulin levels and resistance. Omega-3 fatty acid replacement will improve LPL activity. Exercise especially muscle activation will help “utilize” circulating lipids/fats resulting in lowering triglycerides and VLDL cholesterol.
I don’t know how much was genetic (his father had high triglycerides and premature heart disease) but there was evidence that insulin resistance was contributing to this. Insulin resistance can be modified with dietary changes, fish oil in the diet or as a supplement and avoidance of refined starches (flour), sweets and alcohol.
The answer lies in the immune dysregulation that psoriasis pathophysiology involves. The diagram at the start of this article illustrates the localized rapid immune response our skin can generate in response to environmental insults. Psoriasis involves this response called iSALT (Skin’s Inducible Immune Hub).
The transition from a localized iSALT response in the skin to systemic conditions like psoriatic arthritis (PsA) and atherosclerosis (arterial disease) is often described as the "Psoriatic March." When the iSALT structures in the skin become permanent hubs of inflammation, they stop acting as local guardians and start acting as "leaky" factories that export inflammatory mediators to the rest of the body.
It turns out that our arterial lining cells called the endothelium can take on the same excessive immune response and cell changes that are visibly seen with psoriatic plaques.
The most dangerous consequence of the Psoriatic March is its impact on the cardiovascular system. Researchers often describe the blood vessels of a psoriasis patient as “internalized psoriatic skin.”
Endothelial Dysfunction: Systemic IL-17 and TNF-alpha travel to the arteries and activate the endothelium. This makes the vessel walls “sticky,” allowing cholesterol and inflammatory cells to adhere more easily.
Atherosclerosis as iSALT: In a sense, an atherosclerotic plaque is similar to an iSALT structure. It involves the same recruitment of macrophages and T-cells, but instead of happening in the dermis, it happens in the arterial wall. Chronic skin inflammation accelerates this process, significantly increasing the risk of myocardial infarction (heart attack).
Chronic systemic inflammation from the skin effectively “hijacks” lipid metabolism:
HDL Dysfunction: Psoriasis doesn’t just lower HDL (”good” cholesterol) levels by roughly 15%; it actually oxidizes the HDL, making it dysfunctional. Instead of clearing cholesterol, this oxidized HDL can actually become pro-inflammatory.
Cytokine Interference: High levels of TNF-alpha and IL-6 from the skin’s iSALT hubs interfere with lipase enzymes, leading to higher triglycerides and lower “good” cholesterol. Recall LPL is a lipase (lipid enzyme).
First there is evidence that psoriasis has a polygenic gene association. This means more than one gene variant, and hence functional gene changes can additively contribute to psoriasis as a disease presentation.
As of early 2025, large-scale meta-analyses (including studies with over 800,000 individuals) have expanded the map of psoriasis susceptibility:
32-33 New Risk Variants: Recent GWAS meta-analyses identified dozens of previously unknown loci, bringing the total to over 100 high-confidence genetic regions.
Key New Genes: Research has highlighted AIF1, FCGR3A, and HSPA1A as critical functional variants. These genes are involved in macrophage activation and protein folding stress, suggesting that “genetically driven” psoriasis is as much about how the body handles cellular stress as it is about the T-cells themselves. These genes make the body overreact to minor cellular stress
The summary above is basically informing us that we have genetically determined variants involving our complex immune system and its response to environmental insults, that determine our susceptibility towards the various clinical manifestations of psoriasis.
There are studies/data that indicate that managing the psoriasis can lower the risk of an endothelial (cardiac or other organ arterial disease) event as well as lowering the circulating cholesterol. It has been irrefutably demonstrated that circulating atherogenic non HDL cholesterol molecules have a dose response effect on developing symptomatic plaque and arterial obstruction/thrombosis.
At this point, I now have an understanding and evidence that the patient and I need to address this gentleman’s skin response with equal weight as addressing his cholesterol and lipid results.

Disclaimer: This information is for educational purposes only and is not intended to replace professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.
Southwest Florida’s premier Medical Home. Dedicated to prevention, access, and the patient relationship. Serving Fort Myers, Sanibel, Cape Coral, Bonita Springs, Naples, Punta Gorda & surrounding Southwest Florida areas.
Contact
6160 Winkler Road
Fort Myers, FL 33919
(239) 362-3005
Fax: (239) 362-3392
staff@imlwp.com